The research
The first thing to point out is that we are dealing with a natural experiment over which the researchers have no control. This means the researchers conducting the evaluation are independent of the intervention and have no conflict of interest that would bias them toward producing either positive or negative results. The design of the evaluative study has been adapted to the constraints of the intervention, and the researchers have made efforts to ensure the results will be both useful and usable.
The intervention
The health region of Sahel, located in the northern part of the country, is the region with the worst indicators in the country for both health and healthcare services utilization. Consequently, the Regional Health Department, with the collaboration of Help, decided in September 2008 to implement a trial of user fee exemptions with funding support from ECHO. The NGO concentrated its efforts in two of the region’s four districts, Dori (290,000 inhabitants and 18 healthcare centers in 2009) and Seba (180,000 inhabitants and 11 healthcare centers in 2009).
The key principle is to make healthcare services free at the point of service for vulnerable groups. In return, the COGESs are reimbursed for the costs of providing these services. The NGO acts as a third-party payer, a role that otherwise would fall to the State or a national health insurance.
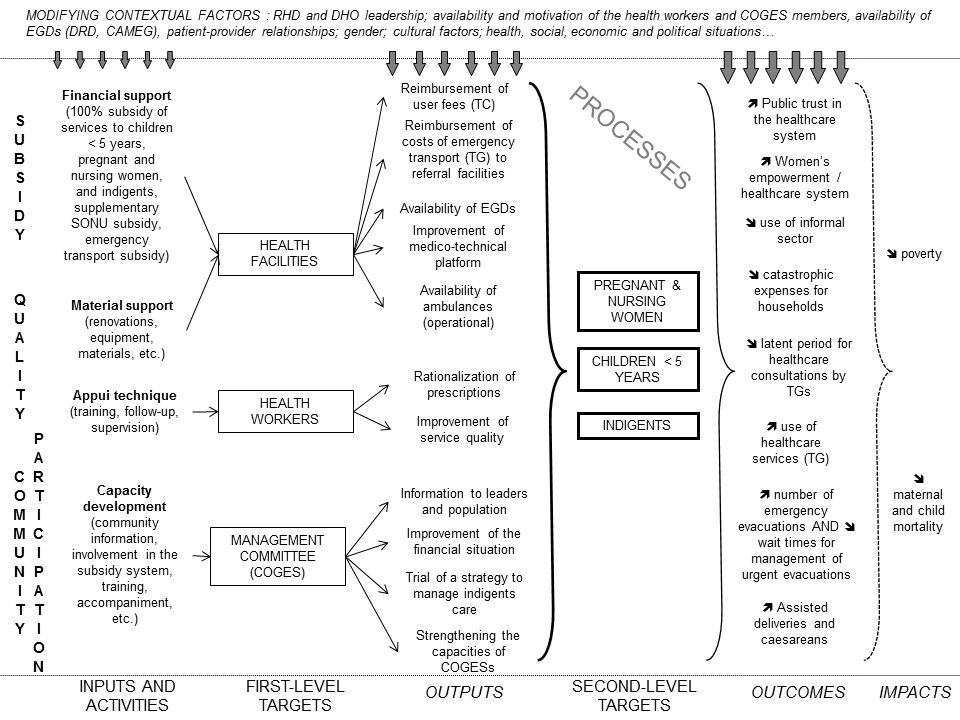
Intervention model
The NGO has implemented a variety of activities to support this exemption measure, in collaboration with the health district teams and the COGESs: information and public awareness campaigns, community mobilization, training for COGES members, training and medical supervision for health workers, reimbursement of medical acts, financial monitoring, etc. Over the short term, the aim of this experiment is to improve access to health and social promotion centers (CSPS) for the three target populations, as well as to strengthen the empowerment of COGESs and the target publics, to improve COGES’ financial positions, and to reduce healthcare expenditures. Over the long term, this intervention should help to improve people’s health and lower households’ risk of falling into poverty.